Goshajinkigan
Efficacy of Goshajinkigan for Peripheral Neurotoxicity of Oxaliplatin in Patients with Advanced or Recurrent Colorectal Cancer Toru Kono,1 Noriaki Mamiya,1,2 Naoyuki Chisato,1 Yosiaki Ebisawa,1 Hirotaka Yamazaki,3 Jiro Watari,4 Yasuhiro Yamamoto,5 Shigetaka Suzuki,5 Toshiyuki Asama,1 and Kazunori Kamiya6 1Division of Gastroenterologic and General Surgery, Department of Surgery, Asahikawa Medical University, 2-1 Midorigaoka-higashi, Asahikawa, Hokkaido 078-8510, Japan 2Division of Cancer Chemotherapy Center, Higashiasahikawa Hospital, Asahikawa, Japan 3Department of Surgery, Kushiro City Medical Association Hospital, Kushiro, Japan 4Deptartment of Gastroenterology, Kushiro City Medical Association Hospital, Kushiro, Japan 5Department of Surgery, Kobayashi Hospital, Kitami, Japan 6Department of Surgery, Karasawa Hospital, Asahikawa, Japan Abstract Peripheral neurotoxicity is the major limiting factor for oxaliplatin therapy. Goshajinkigan (GJG), a traditional Japanese herbal medicine, was recently shown to be effective in protecting against the neurotoxicity of taxanes in Japan. We retrospectively investigated the effect of GJG on peripheral neurotoxicity associated with oxaliplatin therapy. Ninety patients with metastatic colorectal cancer that received FOLFOX4 or modified FOLFOX6 therapy were assigned to receive one of the following adjuncts: oral GJG at 7.5 g day−1 (Gr oup , 𝑛 = 11) intravenous supplementation of calcium gluconate and magnesium sulfate (1 g each before and after FOLFOX) (Group B, 𝑛=14) a combined GJG and calcium gluconate and magnesium sulfate therapies (Group C, 𝑛=21), or no concomitant therapy (Group D, 𝑛=44) the incidence of peripheral neurotoxicity was investigated when the cumulative dose of oxaliplatin exceeded 500 mg m−2. When the cumulative dose of oxaliplatin exceeded 500 mg m−2, the incidence of neuropathy (all grades) in Groups A–D was 50.0%, 100%, 78.9%, and 91.7%, respectively. It was lowest in the group that received GJG alone. Concomitant administration of GJG reduced the neurotoxicity of oxaliplatin in patients that received chemotherapy for colorectal cancer. 1. Introduction In recent years, the standard chemotherapy for advanced/recurrent colorectal cancer is a continuous intravenous infusion of 5-fluorouracil (5-FU) combined with either oxaliplatin (FOLFOX, FOLFOX4 or modified FOLFOX6) or irinotecan (FOLFIRI) [1–3]. Acute and persistent peripheral neuropathy is the characteristic of oxaliplatin therapy [4], and the oxaliplatin dose must be limited to avoid toxicity. The prevalence of peripheral neurotoxicity increases with the total accumulated dose of oxaliplatin, and often interferes with the continuation of FOLFOX therapy [5]. Gamelin et al. [6, 7] reported that administration of calcium gluconate and magnesium sulfate (Ca/Mg) before and after oxaliplatin therapy could alleviate peripheral neurotoxicity. Other similar treatments have been described, including carbamazepine [8–10] or glutathione [11], but an effective remedy for peripheral neurotoxicity related to oxaliplatin therapy has not yet been established. Goshajinkigan (GJG) is an extracted traditional Japanese herbal medicine (Kampo) that is mainly used for the improvement of symptoms like numbness, cold sensation and limb pain associated with diabetic neuropathy [12–15]. Moreover, Mamiya et al. [16] and Shindo et al. [17] recently reported that peripheral neurotoxicity due to oxaliplatin was relieved by administration of GJG in patients with advanced colorectal cancer that were receiving FOLFOX therapy. We conducted the present retrospective study to compare the efficacy of GJG with that of Ca/Mg for alleviation of peripheral neurotoxicity in patients with advanced or recurrent colorectal cancer that received either FOLFOX4 therapy or modified FOLFOX6 (mFOLFOX6) therapy at our hospital and affiliated institutions in Japan. Source : Evidence-Based Complementary and Alternative Medicine Volume 2011 (2011), Article ID 418481, 8 pages doi:10.1093/ecam/nep200 LINK TO FULL ARTICLE 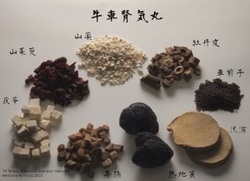 |
|
